


My Brain, My Cartographer
Maps and feelings, real and virtual

Affective Medicine, the name of this blog, looks like Effective Medicine, which is nice. But it sounds quite different; that short A has the emphasis. Affect is jargon from psychology and psychiatry, but even here it’s used differently. In the psychiatric exam, we teach that it’s something like a person’s display and range of emotion. In psychology and neuroscience, affect refers more to a form of qualia, as in “what it’s like to be sad” or “what it’s like to be excited.”
n. any experience of feeling or emotion, ranging from suffering to elation, from the simplest to the most complex sensations of feeling, and from the most normal to the most pathological emotional reactions. Often described in terms of positive affect or negative affect, both mood and emotion are considered affective states.
Notably, this doesn’t really include observable emotion parameters like facial expressions, physiologic changes, and behavior. It’s mostly interchangeable with feelings, core affect, or the delightful “raw feels,” which sounds like the title of a Promise Ring EP.
Understanding how feelings work seems important for psychiatry! Here’s one possibility.
Affect is a composite of many factors
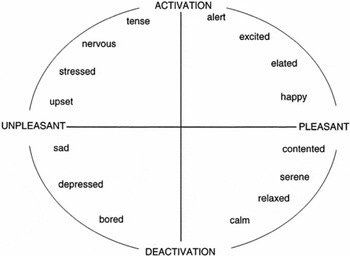
In the standard model, affect has two continuous dimensions. Valence is pleasantness or unpleasantness, while arousal refers to level of alertness or activation. Emotions entail discrete affective states; moods are more general and persistent.
But this division omits something critical: your body! Our most frequent feelings, after all, are mundane needs like being tired, hungry, and having to pee, sometimes known as homeostatic feelings. Consider too that prototypical affects like joy and fear presumably evolved from body states like satiety or air hunger, while severe depression and grief are often described as psychic pain. Finally, I have three children, and I assure you that being tired, hungry, and having to pee are a profound influence on affect, mood, emotion, or whatever you call it.
So I would argue that your affect-state (“How are you feeling?) depends as much on the state of your body as it does on mood or emotions. This actually makes very good sense, because…
The Brain Maps the Body
When I drive around, my brain helpfully creates a sort of internal heads-up display, projecting a real-time map of the city street grid. I gather this experience is not universal, but modeling the world is a core brain function. Vision involves creating a sort of virtual reality of your surroundings. Athletes model physics so they can hit fastballs and skate to where the puck will be. People model other animals, as in theory of mind, and their future-self, as in planning. But before any of this, brains modeled the body.

It’s well-known that parts of the brain lay out a topographic representation of the body. Less familiar is that the body “map” continues down to the insular cortex, nestled within the overhanging frontal and temporal lobes. Just like our motor and sensory strips, the insula "contains topographic interoceptive or viscero-sensory maps" representing balance, pain, temperature, taste, and sensation from internal organs.
The insula is just one of the brain’s body maps, though. Coarser representations first appear all the way down in the brain stem. As with retinal mapping of the visual field, a stable image emerges from peripheral input and carries through the brainstem, thalamus, and cortex.
In short, multiple sites in the brain process interoception, mapping our internal physiological state, just as proprioception tracks our body’s position in space.
Feelings are about the body
Mainstream psychology accepts that emotions are “embodied” in some sense, but the details have been controversial since William James. On one level it’s obvious: the experience of intense fear involves body effects like increased heart rate, muscle tension, and piloerection, which we subjectively experience. This cute study asked participants to create body heat maps for different emotions:

One classic view is that feelings amount to a read-out. Emotions change the body and your brain registers these changes. We learn that different body states correspond to different emotions, and that’s what feelings are. Damasio calls this the “body loop,” because there’s a full circuit in which the brain registers an environmental cue, changes the body, then senses those changes.
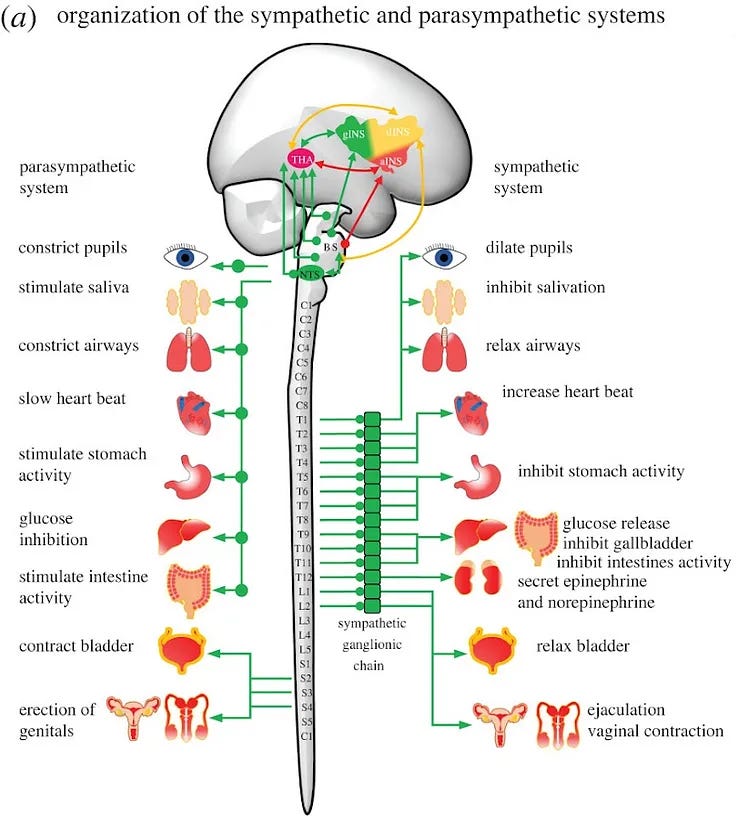
These responses come largely built-in, occur in in deep brain structures, and are implemented via neural maps of different body states:
Subcortical and brainstem systems store neural representations of unlearned motivational drives that are capable of generating innate behavioural repertoires, e.g. consummatory, freezing, approach, avoidance and aggression. Interestingly, these innate behavioural repertoires are also associated with background automatic visceral responses, e.g. increased heart rate, high blood pressure, bowel evacuation, pupil dilation, salivation and sweating, that are thought to elicit basic innate emotions, such as fear, anger, hunger, disgust, happiness, pleasure and surprise. (Fermin, Friston, Yamawaki 2022)
So, what we call feelings are mental representations of different body states (Carvalho and Damasio 2021). Think about the throat and chest tightness of anxiety, the lethargy of depression, the palpitations of panic, the buoyancy of excitement. Think also about the frequent concurrence of medical and psychiatric illnesses, like heart disease and depression. Negative feelings and negative sensations are variations on a theme, different scenes played on the same stage.
The brain generates and simulates feelings
But doesn’t it seem a waste of energy to constantly change your body so much? It’s worthwhile in important situations, like running away from a bear, but a bit overkill for every twinge of anxiety. Also, if emotions and feelings happen in deep brain structures shared by every mammal, what’s the point of our giant cortex?
We usually view emotions as reactions: an organism responds to environmental cues in an adaptive way. Faster reactions are better, and a good way to speed things up is putting common responses into a cache. The insular cortex, more or less, is such a cache. Or, if you prefer, the insula stores “interoceptive trajectories, which can be readily used as interoceptive policies, especially in well-learned environmental situations, for fast generation of interoceptive predictions that evoke visceral responses.” (ibid) Rapid access caching eventually evolved into full-on prediction.
While the mammalian cortex mushroomed its way to human size, greater processing capacity enabled new manipulations of the same old data. The insula gained the ability to store multiple representations: archiving past body maps, comparing different responses to a situation, and modeling future states. This happens wholly in the brain, in the “as-if body loop.”

So, a mature human cortex simulates different body states with its library of neural maps. As a subset of such maps, feelings are also “simulated” by the brain. In Damasio’s words:
as an emotion unfolds, the brain rapidly constructs maps of the body comparable to those that would result were the body actually changed by that emotion. The construction can occur well ahead of the emotional change, or even instead of the change. In other words, the brain can simulate a certain body state as if it were occurring; and because our perception of any body state is rooted in the body maps of the somatosensing regions, we perceive the body state as actually occurring even if it is not.
Errors and Uncertainties
I find these ideas fascinating but, despite being several decades old, they’ve had minimal impact on mainstream psychiatry. In nine years of medical training, I certainly never heard the idea of “feelings as body state maps,” much less the brain as a simulator. Vague references to the mind-body connection don’t count! This is too bad, since there’s a lot of relevance to psychiatric pathology.
Psychosomatic conditions are the obvious one. The varied manifestations of somatization - pain, dizziness, globus, nausea, numbness, fatigue - make a lot of sense seen as body state simulations. They are in fact defined as feelings without actual body change!
Relatedly, many people experience somatization along with anxiety and depression, so much so that the term “SAD Triad” was coined. If we view unpleasant bodily symptoms, anxiety, and depression as just different versions of body maps, this is easy to explain. In fact, we’d expect similar representations to be stored close together, so to speak, and thus for various negative feelings to get activated concurrently, or in lieu of each other.
Somatic delusions, seen in schizophrenia and delusional disorder, are another candidate. People suffer from the idea that they are infested with insects, an organ stopped functioning, or an object is implanted within their body. This sure seems like a malfunction in the body mapping system.
Stepping back, if the “body loop” and “as-if body loop” distinction is valid, it implies that we experience different classes of feelings. Some are actualized in a whole body response, like a full-on startle. Others are enacted virtually in the brain, like mild surprise. There’s presumably a gradient here, as well as some underlying difference in kind.
This fits really well with a common clinical observation. Many patients say they feel bad but don’t present as particularly distraught or impaired. Nowadays we refer to this as “lower-case” or unspecified depression/anxiety. We attribute it to milder symptoms or good coping skills. But perhaps these feelings are of the virtual variety, accounting for their attenuated nature. Other patients project a palpable sense of distress and debility, the “real deal MDD.” There’s just a qualitative difference that’s apparent in the room and isn’t captured by numeric scale. These separate mechanisms could explain the many forme fruste presentations of mental illness.
It makes a lot of sense, engineering-wise, to have different layers of affect. We inherit an ancient high-gain system of fast reactions and big feelings. Consider the toddler. As our cortex develops and the low-gain virtual system comes online, our reactions slow and feelings temper. This helps prevent excessive reactions to unimportant events. One way to see the “as-if loop,” then, is as a buffer or low-pass filter, absorbing much of the noise of the world.
I think this is a fair description of what we mean by stability or wisdom. Instead of controlling or regulating affect, we might see the process of maturation as moving more and more affective experience into our personal brain-based simulation.
Additional Citations
The Archaeology of Mind, Panksepp and Biven, 2012.
Self Comes to Mind, Antonio Damaso, 2010.
“Interoception and Emotion: A Neuroanatomical Perspective” by Bud Craig in The Handbook of Emotion, 2007.